
Breast Cancer

Why should you receive treatment
for breast cancer in AMC ?
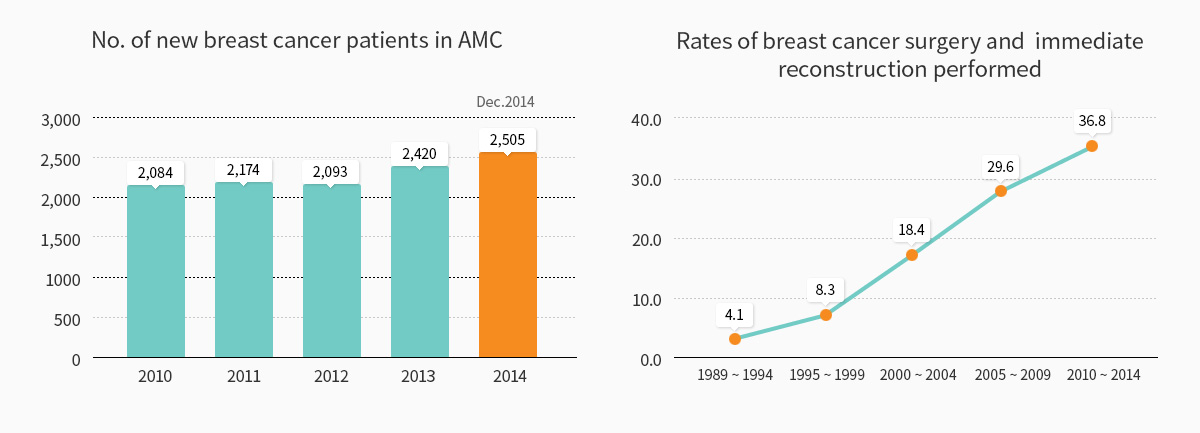
After its opening of the Breast Cancer Clinic in 1992, AMC has expanded the breast cancer clinic to the Breast Cancer Center in 2009, attracting more and more patients every year. The Center was the first nationwide to perform 20,000 breast cancer surgeries by 2013. Currently, it conducts more than 2,000 surgeries a year since 2010 and treats approximately 13% of all breast cancer patients in Korea. About 70% of patients with breast cancer preserve their breast through breast conserving surgery. In addition, by 2014, AMC performed 3,000 breast reconstructions after mastectomy. Also, one in three patients receive mastectomy in conjunction with breast reconstruction.
AMC’s breast cancer team has maximized each patient’s treatment results by providing multidisciplinary treatment through a collaboration system with relevant departments (surgery, medical oncology, plastic surgery, radiation oncology, radiology, pathology, nuclear medicine, and rehabilitation medicine, psychooncology). The Cancer Institute operates five specialized clinics such as the Lifetime Health Clinic (long-term survivor), Preoperative Systemic Treatment Clinic, Young Breast Cancer Clinic, Integrated Treatment Clinic for recurrent cancer, and Hereditary Breast Cancer Clinic, providing optimal medical services suitable to each patient.
Treatment options

Chemotherapy
Normal cells are naturally regulated by our bodies to divide and expire; maintaining a regular number of cells and functions. In contrast, cancer cells are characterized by rapidly growing cells that divide infinitely and unnecessarily, sometimes spreading to other organs.
With this in mind, most anticancer agents are cytotoxic drugs that target these specific characteristics of cancer cells; they aim to stop the metabolic process of fast-growing cells. Unfortunately, anticancer agents cannot decipher the difference between cancer cells and normal cells. Thus, it affects not only the cancer cells but also the normal cells that typically divide rapidly, leading to various adverse effects.

Surgery
1) Mastectomy
Mastectomy is a traditional surgery method used to remove the breast cancer as a whole while simultaneously removing the nipple as well as the axillary lymph nodes. This radical removal is done because breast cancer tends to be multicentric. In other words, cancerous tissues aside from the ones that are palpable may be hiding in a different part of the breast. According to a particular research, the possibility that cancer will remain in another part of the breast depends on its size. The research reports that breast cancers larger than 2 cm have a 38% chance, breast cancers smaller than 2cm have a 26% chance, and breast cancers under the nipple have an 80% chance that the cancer has already spread to a different part of the breast.
The reasons for removing the axillary lymph nodes are as follows: First, cancer cells spread to the lymph nodes in 40% of breast cancer patients so it is desirable to eliminate the axillary lymph nodes to cure the disease completely. Second, a biopsy of the removed lymph nodes reveals whether or not cancer cells have spread to the lymph nodes; this result is available 5-7 days after surgery and will be used for accurate staging of cancer. For instance, if a tumor is smaller than 2 cm and has not spread to the axillary lymph nodes, it is considered stage 1; and if a tumor has spread to the axillary lymph nodes regardless of its size, it is considered stage 2 or higher. Third, knowing how much cancer has spread to the axillary lymph nodes helps determine what treatment options (chemotherapy, radiotherapy, and anti-estrogen therapy) to choose after surgery.
2) Breast conserving surgery
Breast conserving surgery is a surgery method that does not remove the whole breast and instead removes only the cancerous and surrounding tissues. At the same time, the axillary lymph nodes are removed simultaneously by making a new incision under the armpit. The majority of the breast and the nipple will be left intact. When the operation site heals and the patient is discharged from the hospital, the patient will receive radiotherapy at the outpatient clinic. At the outpatient clinic, radiation is applied for five minutes, five times a week for a total of 4-6 weeks. This therapy is used to suppress the growth of microscopic cancers that may remain in the breasts, based on its multicentric tendency.
Among other things, the benefit of breast conserving surgery lies in its cosmetic effects, especially in emotional and psychological satisfaction. Because a vast number of breast cancer patients are young women (60% of AMC breast cancer patients are women in their 30s and 40s), especially in Korea, the demand for breast conserving surgery is high. According to several large-scale studies, there was no significant difference in recurrence and survival rates between breast conserving surgery and mastectomy. For this reason, the number of breast conserving surgery is expected to continually increase.
Radiotherapy
After tumor removal, radiotherapy utilizing various advanced radiotherapy techniques is applied to the remaining breast tissue and/or surrounding lymph nodes, bringing about substantial cosmetic effects and minimal side effects.
1) After breast conserving surgery
Breast conserving surgery, unlike radical mastectomy, is a surgery that preserves the breast while removing the cancer and axillary lymph nodes. Breast cancer has a tendency to be multicentric. This means that there is a 20~30% chance that microscopic cancer cells, invisible to the naked eye, may remain in other parts of the breast although the palpable breast cancer was removed in its entirety,. For this reason, radiation therapy after breast conserving surgery is applied to eradicate microscopic cancer cells. This treatment option is supported by the research findings of the United States’ National Surgical Adjuvant Bowel & Breast Project (NSABP). Research shows that 10 year recurrence rate in breast was 39% after breast conserving surgery without radiotherapy. Meanwhile, breast conserving surgery performed in conjunction with radiation therapy, has a recurrence rate of less than 15% which was similar to that of mastectomy. That is why radiation therapy must be done after breast conserving surgery. Radiotherapy is applied for ten minutes, five times a week. Total duration of radiotherapy is 4 weeks in case of whole breast irradiation only or 6 weeks in whole breast irradiation plus surrounding lymph nodes irradiation, according to the breast cancer status.
2) After mastectomy
Radiotherapy after mastectomy is also performed for patients with advanced breast cancer. Various radiotherapy techniques, such as 3-dimensional conformal radiotherapy, field-in-field technique, intensity modulated radiotherapy, and deep inspiration breath-hold technique are used to minimize side effect.
Endocrine therapy
It is believed that the female hormone estrogen influences the development and growth of most breast cancer cells. Breast cancer cells are known to contain estrogen receptors in the cytoplasm. These receptors bind to the estrogen which causes the cancer cells to grow. Estrogen receptors exist in the cancer cells of around 60-70% of breast cancer patients with menopause, and around 40-50% of breast cancer patients without menopause. Therefore, all patients should be screened for estrogen receptors. If these receptors exist, another substance called Tamoxifen is given to bind to the receptors in place of estrogen, inhibiting the growth of cancer cells. And other drugs, such as LHRH agonists, aromatase inhibitors, fulvestrant and megestrol acetate with/without target agents (everolimus, palbociclib etc) can be used.
Targeted therapy
Substances including various growth factors influence the growth and division process of normal cells and cancer cells. The HER2 (erbb2) gene that typically exists in the body is engaged in controlling cell division. When breast cancer develops, the HER2 gene’s function (overexpression) is activated, promoting the division of cancer cells in some patients. Targeted therapy is a therapy that selectively blocks the cellular pathway of the HER2 gene, which is related to cancer cell proliferation. Unlike conventional anticancer agents, the drugs used for targeted therapy do not cause nausea, hair loss, and cytopenia. The most representative drugs used for the overexpression of HER2/neu in targeted therapy is trastuzumab, pertuzumab, T-DM1 and lapatinib.
AMC's treatment performance
- Excellent results equivalent to advanced countries like the USA
During the last two decades, AMC Breast Cancer Center has shown excellent treatment results in breast cancer patients. Between 1989 and 2008, the five-year survival rate of breast cancer patients of all stages was 89.3%. From 2003 to 2008, the five-year survival rate was 91.9%, a 20% increase compared to that of 15 years ago. Such excellent treatment results are comparable to or better than those of advanced countries such as the United States, Europe, and Japan.
- The largest number of breast cancer surgeries performed in Korea
- 20,000 breast cancer surgeries performed in 2013 for the first time in Korea
- 3,000 breast reconstructions performed in 2014 for the first time in Korea
- 2,500 breast cancer surgeries performed a year on average
- The largest number of breast cancer surgery and immediate reconstruction performed in Korea
- Survival rate of 94-97% in breast cancer patients with stage 1 and 2; Survival rate of more than 80% in breast cancer patient with stage 3